Breast Cancer to Brain Metastases unknown Reboot until Trauma: A Case Report and Literature Review
Download
Abstract
Background: The Aim is to analyze the therapeutic, surgical, and nonsurgical benefits of removing brain tissue that interferes with the patient’s daily routine, while adding conservative hormonal management to the postoperative period.
Case Presentation: We present the case of a 57-year-old woman with a history of left breast cancer (T2N0M0, Stage 2A) who developed neurolgical symptoms secondary to an intracerebral tumor in the right occipital lobe. Initial symptoms included unconsciousness and focal neurological deficits. Imaging revealed a cystic lesion with significant perifocal edema and mass effect. A surgical intervention involving osteoplastic craniotomy was performed, and histopathology confirmed metastasis from breast adenocarcinoma. Postoperatively, the patient exhibited clinical and radiological improvement with a reduction in neurological symptoms and mass effect.
Conclusion: Multidisciplinary care was critical in managing this patient, resulting in symptomatic improvement and positive postoperative dynamics. This case reinforces the importance of tailored treatment plans involving surgery and adjuvant therapies for patients with brain metastases from breast cancer.
Introduction
Breast adenocarcinomas (ACMs) are malignant neoplasms that frequently disseminate both hematogenously and to the brain parenchyma. occurs despite the brain’s lack of a conventional lymphatic drainage system, with metastasis primarily facilitated through the attachment of tumor cells to the endothelium of brain vasculature, allowing their infiltration into the bloodstream [1].
Neuroendocrine tumors, though rare, affect various organs, including the lungs, pancreas, and gastrointestinal tract. Neuroendocrine breast carcinomas constitute a mere 0.5% of cases and were first described in 1977. They exhibit immunohistochemical positivity for neuroendocrine markers in 50% of cases. According to the 2012 World Health Organization (WHO) classification, they are categorized into well-differentiated, poorly differentiated, or invasive carcinomas with neuroendocrine differentiation based on the degree of marker expression [2].
Brain metastases from breast cancer remain a significant clinical challenge, often managed through chemoradiation, which improves systemic disease control. Agents such as cisplatin and vinorelbine have shown efficacy in controlling toxicity and improving therapeutic outcomes in breast cancer patients with brain metastases [3]. Specific sites of metastasis, such as the cerebral fornix, are associated with symptoms like memory deficits, nausea, vomiting, and headaches. Hormone receptor therapies have demonstrated considerable efficacy in cases of breast cancer metastasized to the cerebral fornix [4].
The treatment of breast cancer with brain metastases is complex, depending on factors like tumor characteristics, patient comorbidities, and lesion size, shape, and number. Whole-brain radiotherapy (WBRT) remains a cornerstone of therapy and is frequently combined with surgical resection in appropriately selected patients [5].
Case Presentation
A 57-year-old woman were brought to the emergency department after being found unconscious by a family member who promptly contacted emergency services. On arrival, the patient underwent a comprehensive evaluation. On initial examination, her Glasgow Coma Scale (GCS) score was 7, indicative of significant neurological impairment. Pupillary assessment revealed asymmetry, anisokoria, and sluggish reactivity, which suggested focal neurological deficits. Motor strength was noted to be 3/5 bilaterally, while no abnormalities were observed in cranial nerve function. The patient’s vital signs were stable. Past Medical History: The patient had a complex medical history, including chronic normochromic normocytic anemia of moderate severity and a diagnosis of left breast cancer (T2N0M0, stage 2A) for which she had undergone a left radical mastectomy and eight cycles of chemotherapy. MRI: A series of axial, sagittal, and coronal MRI scans were performed using T1, T2, and FLAIR imaging sequences. The scans revealed a 0.65 cm leftward shift of the midline structures. The posterior horn of the right lateral ventricle was deformed by a cystic lesion located in the right parieto-occipital region, accompanied by pronounced perifocal edema. Diagnosis: Intracerebral mass (tumor) in the right occipital lobe. A stroke was initially suspected, prompting immediate admission for further investigations and preparation for potential surgical intervention. The treatment decision was surgical intervention with an osteoplastic craniotomy. The occipital mass was shown in Figure 1, 2.
Figure 1. a) Magnetic resonance image showing a cystic lesion in the right parieto-occipital region. b) Evidence of pronounced perifocal edema and mass effect, distinguishing the lesion from a porencephalic cyst..
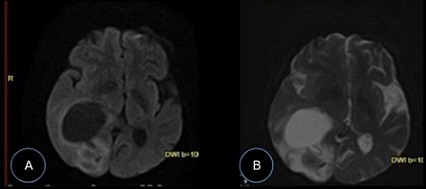
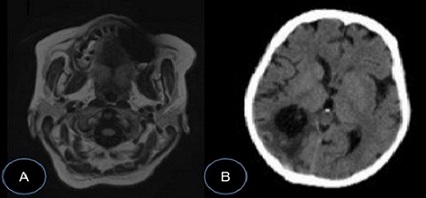
Figure 2. a) Features indicative of cystic-gliotic degeneration in the right parieto-occipital region. b) CT scan Postoperative imaging shows the patient tumor-free the right occipital lobe with partial compression of the right lateral ventricle, with improved visibility of the posterior horn after. A reduction in the degree of ventricular compression is evident.
The objective of this study is to analyze the therapeutic effect of brain metastasis from its origin, improving the patient’s quality of life through the surgical process.
Surgical Approach
The patient underwent osteoplastic craniotomy in the right occipital region for tumor excision. Surgical Approach and Description of the Operation. Patient Positioning and Preparation: The patient was placed prone with the head secured in a Mayfield clamp.
Incision and Exposure: A midline incision was made through the skin and aponeurosis along the projection of the nuchal line. The overlying muscles were carefully retracted with a surgical retractor to expose the occipital bone. A 3 × 3 cm portion of the occipital bone was removed to the right of the nuchal line, starting from the first burr hole.
A 4 cm diameter burr hole was made from a burr hole using a craniotome. The dura mater is taut and nonpulsatile. After the tumor boundaries were clarified by ultrasound (Logic P6 device), the dura mater was opened in a horseshoe shape and the tumor cyst was drained. The contents of the cyst (clear xanthochromic fluid) were taken for cytological examination. Tumor tissue was found in the posterior wall of the cyst, represented by a nodule with inclusions of thrombosed vessels. Using microsurgical techniques, the nodule was excised and sent for histological examination. Hemostasis with fibrillar material. The dura mater is firmly sutured. The bone flap is placed in place and fixed with two craniofixations. The wound is sutured layer by layer. Aseptic etiquette. Closure and drainage: After hemostasis was verified, the dura mater was left open, and sialoplasty was performed with the aponeurosis of the occipital muscle. Protecting of the large blood vessels and functional brain tissues was conducted during the operation. Postoperatively, she received a comprehensive treatment regimen, including antibacterial, anticonvulsant, and hormonal therapies.
Post-Operative Period
Follow-up imaging by CT scan after surgical intervention revealed a reduction in the midline shift to 7.3 mm and a decrease in perifocal edema. A residual cystic cavity with minor hemorrhagic components was visualized in the right occipital lobe. Postoperative imaging revealed signs of pneumocephalus, with a subcutaneous hematoma.
Follow-Up
Following the surgical removal of the intracerebral tumor in the right occipital lobe, the patient was closely monitored in the intensive care unit (ICU). Postoperative CT imaging revealed a reduction in the displacement of midline structures, a residual cystic cavity with hemorrhagic density inclusions, and decreased perifocal edema, consistent with expected postoperative changes. Postoperative management included a multidisciplinary therapeutic approach consisting of antibacterial therapy, anticonvulsant therapy, infusion therapy, hormonal therapy, antihypertensive therapy, and symptomatic treatment. After one month and 3 weeks, the patient was discharged.
Discussion
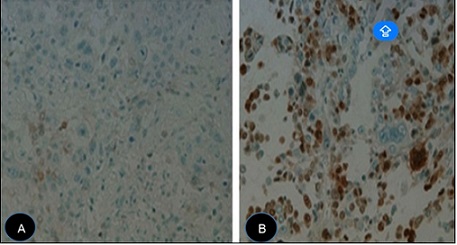
This case highlights the clinical complexity of managing a patient with multiple pathologies, including a history of T2N0M0 stage 2A breast cancer treated with radical mastectomy and recurrent neurological symptoms due to brain metastasis. Although initial imaging findings suggested a pilocytic astrocytoma, histopathology confirmed the lesion as a metastatic adenocarcinoma of breast origin. Shown in Figure 3.
Figure 3. a) Histological image of breast cancer. b) Histological image of brain metastasis due to breast cancer..
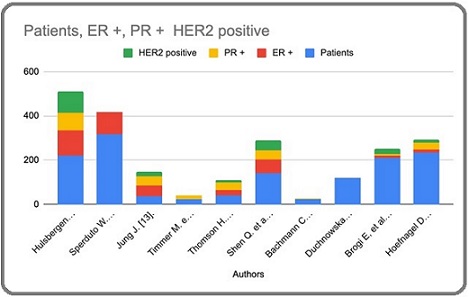
Breast adenocarcinoma is one of the leading malignancies responsible for metastatic dissemination to the brain, often resulting in severe neurological symptoms that impair quality of life and significantly reduce survival. Despite advances in therapy, adenocarcinoma metastases (ACMs) remain a challenging condition, with their ability to invade the brain parenchyma attributed to hematogenous spread and disruption of the blood-brain barrier. This process is regulated by the firm adhesion of tumor cells to the endothelial lining of cerebral vasculature, facilitating transmigration into the brain [6]. A population-based study analyzing the prognosis of 1,302,166 patients with non-hematologic malignancies of the central nervous system (CNS) between 2010 and 2013 identified survival outcomes for various cancers with brain metastases. Metastatic melanoma showed an incidence of 28.2%, lung adenocarcinoma 26.8%, non-small cell lung cancer 25.6%, and small cell lung cancer 23.5%. Breast cancer, and brain metastases were associated with relatively longer survival, ranging from 10 to 12 months, comparable to metastases from bronchoalveolar carcinoma and prostate cancer [7]. Shown in Table 1. Figure 4.
| Authors | Kind of study | Year | Patients | ER + | PR + | HER2 positive |
| Hulsbergen C. et al. [11]. | Multicenter analysis | 2020 | 219 | 117 | 79 | 96 |
| Sperduto W. et al. [12]. | Retrospective | 2020 | 316 | 100 | 40/160 | 22/173 |
| Jung J. [13]. | Retrospective | 2018 | 37 | 47 | 43 | 21 |
| Timmer M. et al. [14]. | retrospective | 2017 | 24 | 12.5 | 16 | 65% |
| Thomson H. et al. [15]. | Retrospective | 2016 | 41 | 22 | 36 | 11 |
| Shen Q. et al. [16]. | Retrospective | 2015 | 140 | 62 | 44 | 44 |
| Bachmann C. et al. [17]. | Retrospective | 2013 | 24 | 50% | 45% | 80% |
| Duchnowska R. et al. [18]. | Retrospective | 2012 | 120 | 29% | 29% | 14% |
| Brogi E, et al. [19]. | Retrospective | 2011 | 209 | 11 | 6 | 25 |
| Hoefnagel D. et al. [20]. | Retrospective | 2010 | 233 | 15 | 32 | 12 |
Figure 4. Graphic of Hormonal Studies Related to Breast Cancer with Brain Metastasis .
Cranial metastases often present with specific manifestations, such as occipital condyle syndrome in breast and prostate cancers, which are among the most common primary tumors to metastasize to the occipital condyle [8]. In cases where patients are diagnosed with large metastatic lesions or experience significant mass effect, surgical resection combined with radiotherapy in regions such as the posterior cranial fossa is essential for managing malignant, symptomatic tumors, regardless of systemic treatment [9] [21].
Studies focusing on HER2-positive breast cancer suggest that such tumors are frequently associated with brain metastases, including both synchronous and metachronous lesions. The metastases have the ability of disseminated tumor cells to colonize distal organs like the brain, which is influenced by their metabolic plasticity and tropism, though the mechanisms underlying this diversity remain an area of active investigation [10].
In conclusion, the patient demonstrated marked enhancement in neurological symptoms and overall well-being following surgical resection and thorough postoperative care. The surgical wound underwent primary intention healing, and the sutures were removed successfully without complications. Postoperative CT images demonstrated positive changes, including a reduction in midline shift and perifocal edema.
A therapeutic regimen was implemented, comprising antihypertensive, disaggregant, and symptomatic therapies, in addition to the gradual mobilization of the patient. Follow-up laboratory and imaging studies, including a contrast-enhanced MRI, are scheduled for one month later. The patient reported no issues regarding the treatment and was provided with explicit guidance for subsequent management. One month after the consultation.
Acknowledgments
Department of Neurosurgery, City Clinical Hospital №68 Gbuz Gkb Im. V.P. Demikhova, Moscow Russia.
Declarations Data Availability
All Data can be requested from the corresponding author.
Conflicts of Interest
There is no conflict of interest.
Informed consent was provided for the patient for this case report.
Ethical Approval
The study adhered to the ethical guidelines outlined in the Declaration of Helsinki for Good Clinical Practice, ensuring informed consent was obtained from all participants. The research was conducted between January 2019 and November 2024 at Moscow City Clinical Hospital №68, Demikhova V.P., Moscow, under Ref. number 1857, dated 02.07.1992, No. 2300-1 (as amended on 06.11.2021).
Funding
None
References
- Breast adenocarcinoma cells adhere stronger to brain pericytes than to endothelial cells Csonti K, Fazakas C, Molnár K, Wilhelm I, Krizbai IA , Végh AG . Colloids and Surfaces. B, Biointerfaces.2024;234. CrossRef
- Neuroendocrine breast carcinoma metastasis to the brain Zanin L, Poliani PL , Liserre R, Panciani PP . BMJ case reports.2019;12(3). CrossRef
- A phase 2 trial of whole-brain radiotherapy combined with intravenous chemotherapy in patients with brain metastases from breast cancer Cassier PA , Ray-Coquard I, Sunyach M, Lancry L, Guastalla J, Ferlay C, Gomez F, et al . Cancer.2008;113(9). CrossRef
- Metastases and Primary Brain Tumors Affecting the Fornix of the Brain Kılıç AE , Yaltırık Bilgin E, Ünal Ö. Cureus.2024;16(4). CrossRef
- Survival outcomes of breast cancer patients with brain metastases: A multicenter retrospective study in Korea (KROG 16-12) Kim JS , Kim K, Jung W, Shin KH , Im S, Kim H, Kim YB , et al . Breast (Edinburgh, Scotland).2020;49. CrossRef
- Breast adenocarcinoma-derived exosomes lower first-contact de-adhesion strength of adenocarcinoma cells to brain endothelial layer Fazakas C, Kozma M, Molnár K, Kincses A, Dér A, Fejér A, Horváth B, et al . Colloids and Surfaces. B, Biointerfaces.2021;204. CrossRef
- Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: a population-based study Cagney DN , Martin AM , Catalano PJ , Redig AJ , Lin NU , Lee EQ , Wen PY , et al . Neuro-Oncology.2017;19(11). CrossRef
- Occipital Condyle Syndrome As the Initial Presentation of Recurrence of Metastatic Breast Cancer: A Case Report Arivazhagan S, Parthiban GP , Busa V, Negulescu C. Cureus.2023;15(2). CrossRef
- Breast Cancer with Brain Metastasis: Molecular Insights and Clinical Management Ivanova M, Porta FM , Giugliano F, Frascarelli C, Sajjadi E, Venetis K, Cursano G, et al . Genes.2023;14(6). CrossRef
- Metabolic diversity within breast cancer brain-tropic cells determines metastatic fitness Parida PK , Marquez-Palencia M, Nair V, Kaushik AK , Kim K, Sudderth J, Quesada-Diaz E, et al . Cell Metabolism.2022;34(1). CrossRef
- Subtype switching in breast cancer brain metastases: a multicenter analysis Hulsbergen AFC , Claes A, Kavouridis VK , Ansaripour A, Nogarede C, Hughes ME , Smith TR , et al . Neuro-Oncology.2020;22(8). CrossRef
- Estrogen/progesterone receptor and HER2 discordance between primary tumor and brain metastases in breast cancer and its effect on treatment and survival Sperduto PW , Mesko S, Li J, Cagney D, Aizer A, Lin NU , Nesbit E, et al . Neuro-Oncology.2020;22(9). CrossRef
- Discordances in ER, PR, and HER2 between primary breast cancer and brain metastasis Jung J, Lee SH , Park M, Youn JH , Shin SH , Gwak HS , Yoo H. Journal of Neuro-Oncology.2018;137(2). CrossRef
- Discordance and Conversion Rates of Progesterone-, Estrogen-, and HER2/neu-Receptor Status in Primary Breast Cancer and Brain Metastasis Mainly Triggered by Hormone Therapy Timmer M, Werner J, Röhn G, Ortmann M, Blau T, Cramer C, Stavrinou P, et al . Anticancer Research.2017;37(9). CrossRef
- Changing molecular profile of brain metastases compared with matched breast primary cancers and impact on clinical outcomes Thomson A. H., McGrane J., Mathew J., Palmer J., Hilton D. A., Purvis G., Jenkins R.. British Journal of Cancer.2016;114(7). CrossRef
- Breast cancer with brain metastases: clinicopathologic features, survival, and paired biomarker analysis Shen Q, Sahin AA , Hess KR , Suki D, Aldape KD , Sawaya R, Ibrahim NK . The Oncologist.2015;20(5). CrossRef
- Receptor change-clinicopathologic analysis of matched pairs of primary and cerebral metastatic breast cancer Bachmann C., Grischke E. M., Staebler A., Schittenhelm J., Wallwiener D.. Journal of Cancer Research and Clinical Oncology.2013;139(11). CrossRef
- Conversion of epidermal growth factor receptor 2 and hormone receptor expression in breast cancer metastases to the brain Duchnowska R, Dziadziuszko R, Trojanowski T, Mandat T, Och W, Czartoryska-Arłukowicz B, Radecka B, et al . Breast cancer research: BCR.2012;14(4). CrossRef
- Breast carcinoma with brain metastases: clinical analysis and immunoprofile on tissue microarrays Brogi E., Murphy C. G., Johnson M. L., Conlin A. K., Hsu M., Patil S., Akram M., et al . Annals of Oncology: Official Journal of the European Society for Medical Oncology.2011;22(12). CrossRef
- Receptor conversion in distant breast cancer metastases Hoefnagel LDC , Vijver MJ , Slooten H, Wesseling P, Wesseling J, Westenend PJ , Bart J, et al . Breast cancer research: BCR.2010;12(5). CrossRef
- Letter to the Editor Regarding "Minimally Invasive Surgery for Spinal Metastasis: A Review" Poullay Silven M, Encarnación-Santos D, Volovish A, Nicoletti GF , Iacopino DG , Valerievich K. World Neurosurgery.2024;184. CrossRef
License

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Copyright
© Asian Pacific Journal of Cancer Care , 2025
Author Details
How to Cite
- Abstract viewed - 0 times
- PDF (FULL TEXT) downloaded - 0 times
- XML downloaded - 0 times